

This article was first published by RNZ
Māori health providers say the disproportionate impact syphilis is having on Māori and Pasifika babies is due to a culturally unsafe and unaffordable primary health sector.
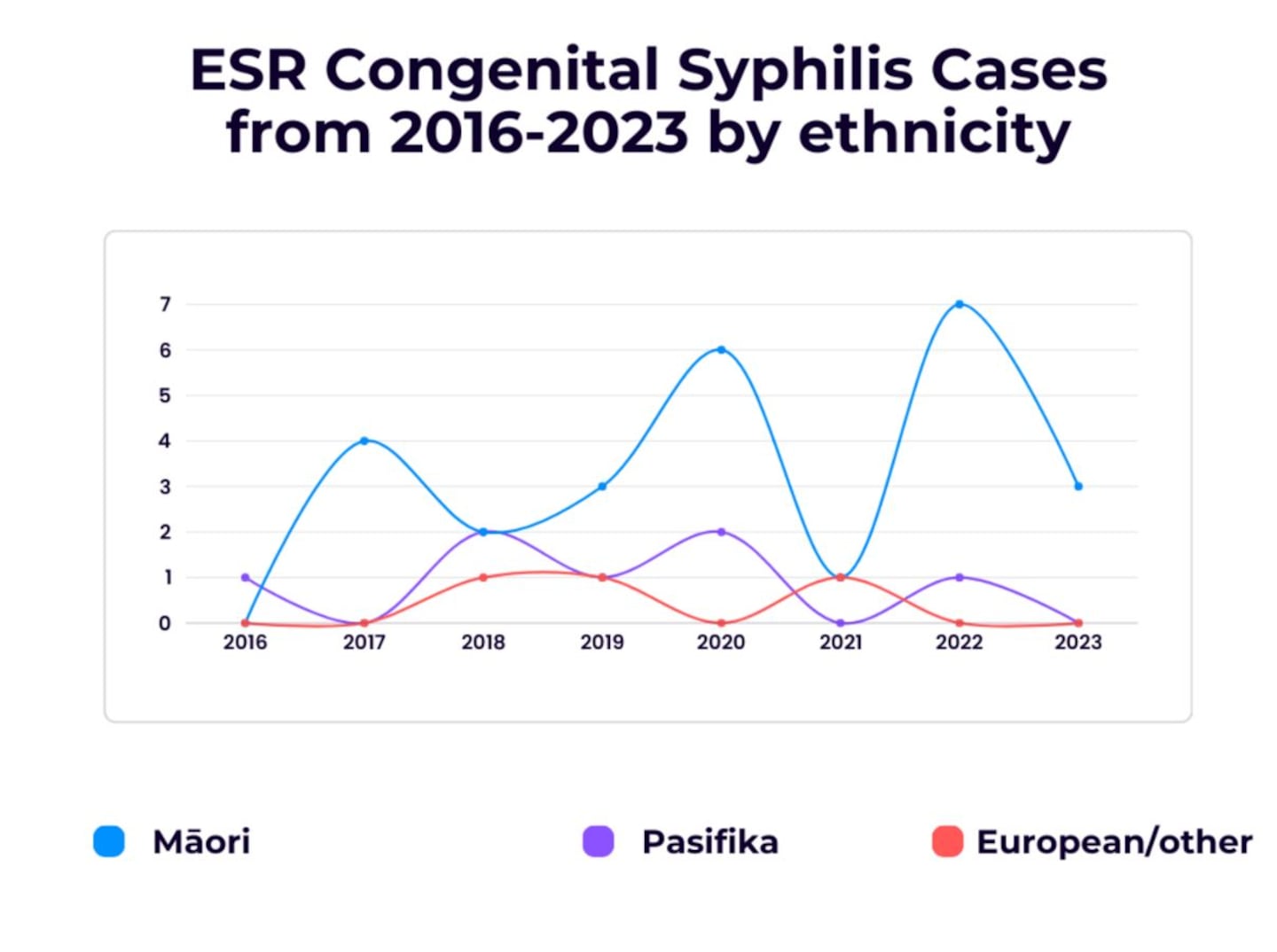
Rates of the disease are on the rise and hitting Māori and Pasifika the hardest.
In the past seven years, the Institute of Environmental Science and Research (ESR) has reported 35 cases of congenital syphilis, where the disease is passed on to a baby through the mother.
A staggering 32 of these were Māori or Pasifika.
The consequences of transmission are serious, possibly causing stillbirth, early birth, and very sick newborns.
The Ngā Maia Trust advocates for better midwifery services for Māori, and its general manager, Tamara Karu, have written recommendations for reducing the incidence of syphilis amongst Māori and Pasifika.
“Transformative Tiriti honouring actions that give practical effect to Te Tiriti o Waitangi are crucial in improving sexual health outcomes for Māori and Pasifika communities,” she said.
Karu suggests the increase and restoration of sexual health services, reducing financial barriers to primary care, and building genuine partnerships with Māori and Pasifika providers.
Actively involving these communities in healthcare decision-making processes to ensure services are culturally and contextually appropriate is paramount.
“Established and effective kaupapa Māori programs such as Hapū Wānanga are being eroded by funding constraints, despite the outcomes being a high priority to populations at higher risk of mortality.
“Addressing these challenges and implementing these recommendations, it is possible to reduce the incidence of syphilis and improve overall health outcomes for Māori and Pasifika communities in New Zealand.
“But the task of turning the situation around is being made more difficult by a huge shortage of midwives, something that is further compounded by a scarcity of those claiming Māori or Pasifika heritage.”

In 2018 the New Zealand College of Midwives showed 25 percent of Aotearoa’s birthing population identified as Māori, and 10 percent as Pasifika.
But in 2021, less than 10 percent of midwives identified as Māori and less than three percent as Pasifika.
That same year the Ministry of Health provided $6 million in funding over the next four years, to increase recruitment of Māori and Pasifika undergraduate midwifery students.
Māori midwifery advisor at the College of Midwives, Te Paea Bradshaw, said it was concerned about the increase of cases of this entirely preventable disease.
“And we also recognise the inequities within those whānau who are affected by this,” she said.
Though underlying causes are varied, Bradshaw said they often occurred due to an intersection of risk factors like health literacy, social deprivation, and access to culturally safe health services.
“And sadly, it is often the communities with the greatest need that have the least access. As a health system, this needs to be corrected.”
Bradshaw said sexual health was a key aspect of midwifery care.
“We know access to care enables early detection, and subsequently the ability to treat, which will prevent the congenital effects to baby.”
But overall, Bradshaw said access to culturally safe health services was crucial.

The president of the Australasian chapter of sexual health medicine, Dr Massimo Giola, said “the only acceptable number of congenital syphilis cases in a country like New Zealand should be zero”.
And since syphilis is diagnosed and treated by a blood test and a couple shots of penicillin, Dr Giola said every single case is a system failure indicator.
“All our leaders in health and politicians should really be jumping up and down every single time there’s a congenital syphilis case.”
Although syphilis screening is always conducted early in pregnancy, it can miss early infections or those acquired later.
To catch this, syphilis testing is repeated later in pregnancy, but only if you live in the North Island.
Because there are fewer cases in the South Island, testing there only happens once, unless risk-factors present themselves.

Giola is calling for change.
“We should all be aware of the inequities and make sure we compensate by allowing those affected populations to access prompt testing and treatment,” he said.
“There should be a mix of low cost and accessible GP practices, but also culturally appropriate services, perhaps marae based or something that Māori and Pasifika people are comfortable accessing.”
Bradshaw and Giola urged all pregnant women to make contact with a midwife and not to wait for symptoms of syphilis, just get a blood test done.
By Elsie Williams for RNZ
